Eighteen Pages. You Understand the First Paragraph.
Nandini had waited four weeks for the report. She had answered every question in the assessment, had sat with her daughter through every session. The report arrived on a Friday afternoon. By page three she had encountered: standard score, percentile rank, confidence interval, working memory index, phonological processing, processing speed, clinically elevated T-score, intraindividual discrepancy analysis, and executive function deficit.
She read the diagnosis on page one. She read the recommendations on page sixteen. The twelve pages in between remained largely opaque.
'What do I do with this?' she asked me.
This blog is the answer — a complete, plain-language guide to every section of a child psychological assessment report.
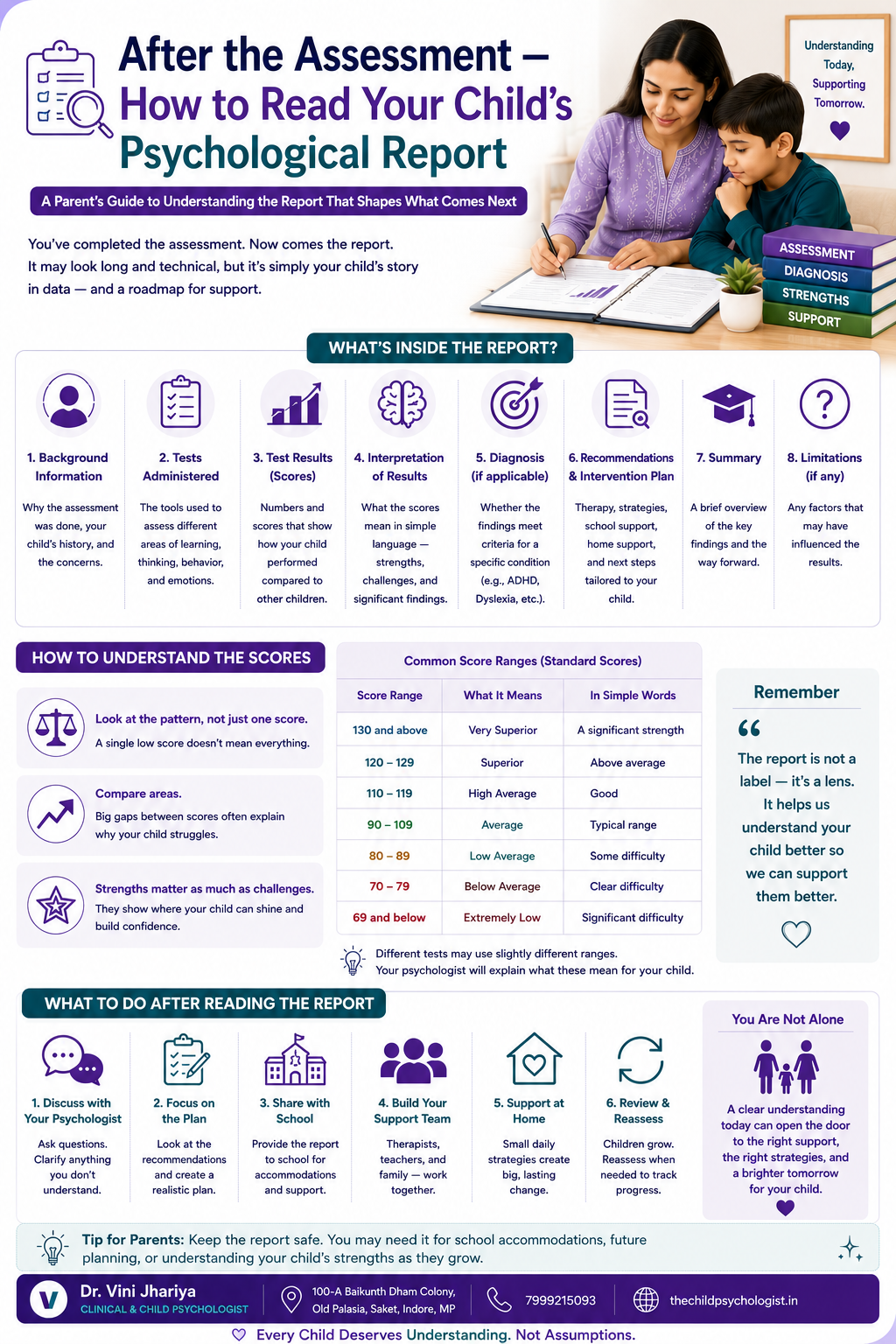
How the Report Is Structured
Page 1 — Identifying information and reason for referral
Pages 2–4 — Background and developmental history (read carefully — check for factual accuracy)
Page 4–5 — Assessment tools used (list of standardised tests administered)
Pages 5–7 — Behavioural observations (how your child presented during testing)
Pages 7–14 — Test results (the section most parents find most overwhelming — explained below)
Pages 14–15 — Summary and clinical impressions (often the most readable section after recommendations)
Pages 15–17 — Diagnosis
Pages 17–18 — Recommendations (the most practically important section)
Understanding Scores — The Complete Guide
Standard Scores
Standard scores compare your child's performance on a specific task to a large sample of children the same age. The scale is constructed so that 100 is exactly average and most children (about 68%) score between 85 and 115.
130 and above — Very superior: Top 2% of children this age
120–129 — Superior: Top 9%. Clearly above average.
110–119 — High average: Above the midpoint. Stronger than most peers.
90–109 — Average: Typical range. Where most children fall.
80–89 — Low average: Below the midpoint but within a common range.
70–79 — Borderline: Significantly below what is typical for this age.
Below 70 — Extremely low: Well below average. Likely producing significant real-world difficulty.
Important: a standard score tells you where your child's performance falls relative to peers — not whether they are 'good' or 'bad' at something. A score of 85 in working memory means working memory is below average for peers — not that the child is unintelligent or incapable.
Percentile Ranks
A percentile rank tells you what percentage of same-age children scored below your child on a given measure.
Percentile 50: Exactly average — half of peers scored below, half above
Percentile 84: Above average — 84% of peers scored below
Percentile 16: Below average — only 16% of peers scored lower
Percentile 5: Well below average — only 5% of peers scored lower
Critical misunderstanding: a percentile rank is NOT the same as a test percentage. A score at the 25th percentile does not mean your child got 25% of the questions right. It means they performed better than 25% of same-age peers — which is below average, but not as catastrophic as '25%' sounds.
Confidence Intervals
You will often see a score presented as a number with a range in brackets — for example: Working Memory Index: 82 (76–88). The range in brackets is the confidence interval. It means the assessor is confident that your child's true score falls somewhere within this range because all psychological tests have some measurement error. Look at the midpoint of the range — the number before the bracket — as the best estimate of where your child's true performance falls.
T-Scores — Used for Behavioural Rating Scales
T-scores are used specifically for behavioural rating scales — the questionnaires completed by you and your child's teacher. They use a different scale from standard scores:
T-score 50: Exactly average
T-scores 60–65: Elevated — above what is typical
T-scores above 65: Clinically significant — clearly outside the typical range
T-scores above 70: Highly elevated — in the range associated with significant clinical concern
When the report says a T-score is 'clinically elevated' or 'clinically significant,' it means the rated behaviours are clearly outside what is typical for a child this age — not a borderline finding.
What the Major Cognitive Measures Mean
Full Scale IQ (FSIQ) or General Ability Index (GAI):
The overall cognitive ability composite — a summary of intellectual functioning. In child assessment, it matters primarily as a baseline: it tells you what your child is intellectually capable of, against which their academic performance can be compared.
Verbal Comprehension Index (VCI):
Measures the ability to understand and use language — vocabulary, verbal reasoning, general knowledge. Frequently intact or above average in children with ADHD or dyslexia — which is part of why their other difficulties are so confusing to teachers who hear them speak fluently.
Fluid Reasoning Index (FRI):
Measures the ability to solve novel problems, identify patterns, and reason without relying on previously learned knowledge. Also frequently intact in ADHD and dyslexia.
Working Memory Index (WMI):
Measures the ability to hold information in mind while using it — the mental scratchpad. One of the functions most consistently affected in ADHD. A low WMI explains why a child forgets instructions moments after hearing them, loses track mid-task, and needs things repeated.
Processing Speed Index (PSI):
Measures how quickly and efficiently the brain processes simple information. A low PSI means the child works more slowly than peers — not due to lower intelligence but due to slower information processing. Explains why a child cannot keep pace with classroom instruction and takes significantly longer to complete tasks than peers of similar intelligence.
Phonological Processing:
Not a WISC index but a separate assessment domain — measures the ability to connect letters to sounds and manipulate the sounds of spoken language. The neurological core of reading. A low phonological processing score alongside low reading scores is the diagnostic signature of dyslexia.
What the Diagnosis Section Is Saying
Common diagnoses you may see:
Autism Spectrum Disorder (ASD) — with specification of support level (Level 1, 2, or 3) and co-occurring conditions
Attention Deficit Hyperactivity Disorder (ADHD) — with specification of presentation (predominantly inattentive, predominantly hyperactive-impulsive, or combined)
Specific Learning Disorder — with specification of the impaired domain: reading (dyslexia), written expression (dysgraphia), mathematics (dyscalculia), and severity specified as mild, moderate, or severe
Anxiety Disorder, Adjustment Disorder, or other emotional conditions — if the assessment identifies significant emotional or behavioural co-occurring conditions
'Within normal limits' or 'no diagnosis indicated' — also a valid and useful outcome. A comprehensive assessment that finds no specific diagnosis still provides a cognitive profile and may identify areas of relative weakness that benefit from support.
Reading the Recommendations Section
This is the section most parents skip to first — and the one most worth reading slowly. Recommendations are specific to your child's profile. If they could have been written for any child, the report is not a good comprehensive report.
School accommodations:
Extended time, preferential seating, written instructions, movement breaks, spelling not penalised. These form the basis of your formal accommodation request under RPWD Act 2016.
Examination board accommodations:
Extra time, scribe, reader, or other provisions for board examinations. These must be applied for through the school with the report as supporting documentation.
Therapy recommendations:
Each should link to a specific finding in the report. If a recommendation is not connected to a specific finding, ask the assessor why it is being recommended.
Medical referrals:
If medication evaluation is recommended, this is a referral to a child psychiatrist or developmental paediatrician — not an immediate prescription.
Reassessment:
When to reassess and why. Standard is typically two to three years, or when the child's educational context changes significantly.
What to Do With the Report — Practically
Read the recommendations section in full — this tells you specifically what action is needed
Book a feedback session with the assessor if one has not been scheduled
Share the recommendations section with the school and write a formal accommodation request citing the RPWD Act 2016
Book any therapy or clinical appointments recommended — do not defer these
Contact the school examination coordinator immediately about board accommodation deadlines
If medication evaluation is recommended, book an appointment with a child psychiatrist or developmental paediatrician — not a GP
File the report safely — you will need it multiple times (school, examination boards, disability certification, future clinical appointments)
If you would like help understanding your child's report or planning the next steps, reach out through thechildpsychologist.in or call 7999215093.
Frequently Asked Questions
Q: What does a standard score of 80 mean in a child psychological report?
A standard score of 80 falls in the low average range — below the midpoint of 100 but within a range that is not uncommon. In context: a standard score of 80 on working memory, alongside higher scores on verbal reasoning, is consistent with the cognitive profile seen in ADHD, where specific processing functions are weaker than general intellectual ability.
Q: What does 'clinically significant' mean in a psychological report?
Clinically significant means the finding is clearly outside the typical range and warrants clinical attention. On rating scales, a T-score above 65 is typically described as clinically significant. It does not mean the child is severely impaired — it means the finding is meaningful enough to inform diagnosis and treatment planning.
Q: What should I do first after receiving my child's psychological report?
Read the recommendations section carefully. Book a feedback session with the assessor. Take school accommodation recommendations to the school in writing, citing the RPWD Act 2016. Book any therapy or clinical appointments recommended. Contact the school examination coordinator about board accommodation deadlines if relevant. File the report safely — you will need it multiple times.
Q: The report says my child has a 'significant intraindividual discrepancy.' What does this mean?
An intraindividual discrepancy means there is a meaningful difference between different scores within your child's own profile — larger than would be expected by chance. For example, a significant discrepancy between high verbal comprehension and low working memory means these two functions are performing at meaningfully different levels. In the context of ADHD or dyslexia, this pattern — high reasoning with low processing-specific scores — is the neurological explanation for why the child seems capable but underperforms.
Q: Can I share my child's psychological report with their school?
Yes — you own the report and can share it. The recommendations section is the most relevant part for the school. For accommodation requests, share the full report along with a formal written request citing the RPWD Act 2016.
Q: My child's report says 'within normal limits' — does this mean there is nothing wrong?
'Within normal limits' means the assessment findings do not indicate a specific neurodevelopmental condition or significant cognitive deficit. This is a valid outcome — not a failure. It means the assessor has ruled out specific conditions and can direct attention toward other explanations for the child's difficulties.
If You Are in Indore or Nearby
If you are based in Indore, Bhopal, Ujjain, Dewas, or nearby areas, Dr. Vini Jhariya is available for in-person consultations. For families outside Indore — across India and internationally — online consultations are available through thechildpsychologist.in.
Address: 100-A Baikunth Dham Colony, Old Palasia, Saket, Indore, Madhya Pradesh
Phone: 7999215093
Website: thechildpsychologist.in
The Report Is a Map — Use It
Nandini came back three weeks after receiving the report. She had read it twice more. She had written notes on the recommendations. She had drafted a letter to the school. She had booked a speech therapy assessment.
'I still don't understand every score,' she said. 'But I understand what the report is telling me about my daughter. And I know what to do with it now.'
That is what understanding the report gives you. Not perfect clinical literacy. The ability to act — specifically, confidently, in the right direction. Reach out through thechildpsychologist.in or call 7999215093.